Mysteries of the Hearing Brain

The Mysteries of the Hearing Brain
The audiologist may view every new patient as a potentially interesting mystery, waiting to be solved. Even a seemingly routine diagnosis of presbycusis does not always provide an adequate explanation for the nature of the hearing difficulties presented by some patients. After twenty-six years of audiological practice, Dr. Samira Anderson decided to pursue better approaches or tools to uncovering mysteries of hearing difficulties that are not apparent on the audiogram, and she obtained a PhD in Auditory Neuroscience. In this new column she aims to connect recent research advances to clinical practice. Her research continues to be driven by her clinical experiences, and she invites readers to submit their questions or experiences for potential future articles.

Age-related hearing loss is associated with isolation, depression, and a decline in cognitive function.1,2 And, loneliness and loss of memory are among the top fears experienced by senior citizens. Yet, hearing loss remains an untreated deficit in the majority of individuals who would benefit from intervention. Perhaps the knowledge that hearing aid use may offset or even improve neural and cognitive function may be the incentive needed to pursue help for hearing loss. Indeed, some hearing aid manufacturers have begun to capitalize on the link between hearing loss and cognitive decline in their advertisements.
Is there any evidence that supports the efficacy of hearing aid use for improving cognitive function? Yes, there is some indication that hearing aid use has benefits beyond improved hearing ability. A 25-year longitudinal study compared the course of cognitive decline (assessed using the Mini-Mental State Examination3) in 3670 participants ages 65 and older who self-reported moderate or major hearing loss to cognitive decline in participants who self-reported no hearing loss.4 The investigators found that (1) the rate of cognitive decline was steeper in individuals with untreated hearing loss than in individuals who reported normal hearing, and (2) the rate of cognitive decline in individuals who wore hearing aids was equivalent to the rate in the group who reported no hearing difficulty. They concluded that hearing aid use may offset cognitive decline.
In my October 2018 column, I described a study funded by the Hearing Health Foundation to evaluate the effects of amplification on auditory neural function in new hearing aid users ages 60–85, both at the time of fitting and over the course of six months. We also evaluated changes in cognitive function, specifically working memory, processing speed, and attention/inhibition after six months of hearing aid use. The experimental group of participants (N=18, 8 males) who wore hearing aids were matched in age, hearing loss, and IQ to a group of non-hearing aid users (N=14, 5 males). All of the participants in the study had mild to moderate sensorineural hearing loss, were free of neurological disorders, and passed a dementia screening.5
Both experimental and control groups of participants were fit bilaterally with Widex Dream 440 Fusion hearing aids. Cognitive testing was performed while the participants were wearing hearing aids, and cortical auditory-evoked responses were recorded to a speech syllable /ga/ presented in sound field in aided and unaided conditions. The experimental group wore their hearing aids a minimum of eight hours a day for six months, but the control group did not wear hearing aids during this time. After six months, both groups returned for repeat cognitive testing and cortical recordings.
The results showed that cortical amplitude increased in the hearing aid group, particularly for the N1 and P2 peaks, which reflect attention and auditory object identification, respectively (Figure 1). No similar changes were noted in the control group. Similarly, working memory scores improved significantly in the hearing aid group (average increase of 8.5 in the standard score), but the scores did not improve in the control group (average decrease of 2.3 in the standard score). No changes were seen in the processing speed or attention/inhibition scores. Interestingly, changes in P2 amplitude were positively correlated with changes in working memory. These findings suggest that improved neural processing and ease of listening through the use of hearing aids may free up brain resources that can be allocated for memory.
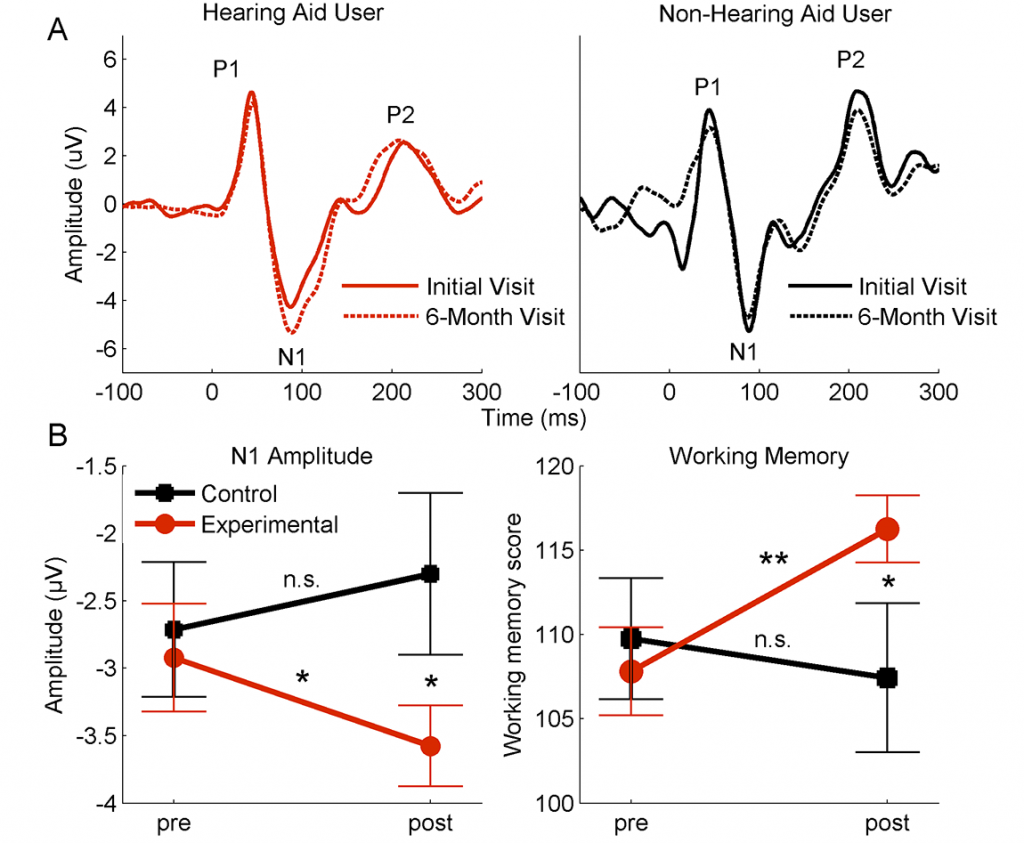
Figure 1. A. Aided cortical waveforms from an individual who used hearing aids (red) and an individual who did not use hearing aids (black) recorded during initial (solid line) and 6-month (dashed line) follow-up visits. The N1 and P2 peak amplitudes are larger after six months of hearing aid use, but change was not noted in the non-hearing aid user. B. Left panel: Group average cortical N1 amplitudes in the control (no hearing aid use, black) and experimental (hearing aid use, red) at the initial and final visits. Right panel: Group average working memory scores in the control and experimental groups at the initial and final visits. Note that the groups are matched on the cortical and working memory measures at the initial visit, but the experimental group improved on both of these measures while the control group did not change. *p < 0.05, **p < 0.01. Errors bars: 1 Standard Error
We hope that for individuals with age-related hearing loss, our study and future studies will provide additional motivation to pursue help for their hearing difficulties. On average, individuals wait seven years from the time they first notice hearing difficulty until they seek help. Perhaps the knowledge that hearing aid use may improve memory ability, in addition to improved hearing ability, will shorten this delay.
References
- Heine C and Browning CJ. Communication and psychosocial consequences of sensory loss in older adults: overview and rehabilitation directions. Disabil Rehab 2002;24(15):763–73.
- Lin F, Yaffe K, Xia J, et al. Hearing loss and cognitive decline in older adults. J Am Med Assoc Int Med 2013;173(4):293–99.
- Folstein MF, Folstein SE, and McHugh PR. Mini-mental state : A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189–98.
- Amieva H, Ouvrard C, Giulioli C, et al., Self‐reported hearing loss, hearing aids, and cognitive decline in elderly adults: a 25‐year study. J Am Geriatr Soc 2015;63(10):2099–104.
- Karawani H, Jenkins K, and Anderson S. Restoration of sensory input may improve cognitive and neural function. Neuropsychologia Jun;114:203–13. doi: 10.1016/j.neuropsychologia.2018.04.041. 2018.