A Treatment Planning Checklist

The Wired Audiologist
Peter Stelmacovich, MCl Sc, is a hard of hearing audiologist who works for a Canadian manufacturer. In Peter’s column, The Wired Audiologist, he discusses many of the issues that affect him personally as both a hard of hearing consumer and an audiologist.
In my last column I discussed the value and importance of incorporating Speech in Noise testing into an audiologist’s standard set of assessments. How can one now develop a treatment plan with this information?
My proposal for treatment planning has been influenced in part by Sergei Kochkin’s paper on the “multiple environmental listening utility” or MELU (http://old.betterhearing.org/pdfs/kochkin_hearingjournal1107.pdf). In this paper, Dr. Kochkin argues that “overall satisfaction with hearing aids will not reach a respectable 80% level until consumers are at least “somewhat” satisfied with their hearing aids in at least 70% of the listening environments important to them.”
Currently, we have a number of treatment options available for patients with hearing loss. These include:
- Amplification of various styles and power.
- Telecoils incorporated into the hearing instrument.
- Directional microphones incorporated into the hearing instruments
- Bluetooth devices including streamers, microphones, and television interfaces.
- Frequency modulated fixed gain wireless transmission systems.
- Digital fixed gain wireless systems.
- Adaptive gain digital wireless systems.
- Cochlear implantation.
- Implantable bone conduction and middle ear devices.
All of these have potential utility and value for patients with hearing loss. Some are important for restoring audibility of speech sounds, while others are designed to improve the signal-to-noise ratios (SNR). Both the restoration of audibility and the enhancement of SNR are needed by most patients with hearing loss. Our job is to select the right combination of equipment in conjunction with appropriate counseling and training in order to help our patients communicate in the listening environments encountered in the real world.
Prior to developing the treatment plan, we need, at the very least, the following information:
- The audiogram.
- Word identification scores in quiet.
- Speech-in-noise testing.
- Assessment of environments which are important to the client (e.g., COSI).
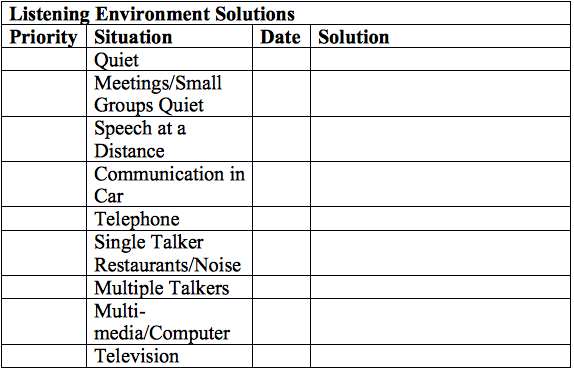
With at least this information, we can now develop a plan for the client. Below is my proposed planning tool that can help with the selection of the equipment:
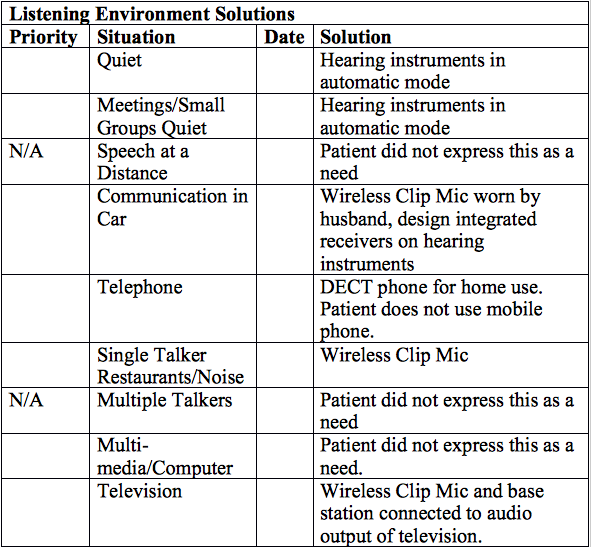
Let us take a look at some examples of how this tool can be used. The first is an 84-year-female with mild to moderate sensorineural hearing loss bilaterally. Word identification in quiet was 80% and 84% for right and left ears respectively. The patient initially tried a Bluetooth microphone and streamer but found it too complex. Moreover, the patient continued to express difficulties hearing in background noise despite having ear level directional microphones. Hearing-in-noise testing was performed using the LiSN-S PGA and results showed that this patient had significant difficulties hearing in background noise requiring the use of a wireless system. Design integrated receivers were added to the clients hearing aids and an easy to use wireless clip mic was selected.
While this example involved the use of wireless microphones, it is conceivable that other patients with a similar audiogram will perform better on the LiSN-S PGA and thus will derive benefit from advanced directional microphones on the hearing instruments and Bluetooth microphones. We need to remember that the audiogram on its own is not a good predictor of speech perception in noise (See Kraus and Anderson, Hearing Journal: July 2013 - Volume 66 - Issue 7 - p 36) and as such it is not surprising that this older patient required more than ear level directional microphones.
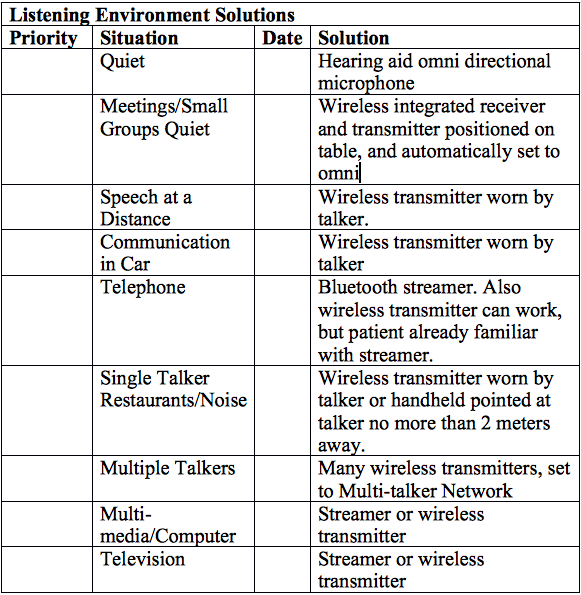
The second is a client that I assisted about 6 months ago. He is in his 60s and a business executive. He has a profound loss in his left ear and a moderate-severe sensorineural loss in his right ear. Word identification score was 0% in his left ear and 84% in his right ear. Hearing-in-noise testing was not performed in this case, but he reported significant difficulties in understanding speech in background noise even with the use of a directional microphone on his right hearing aid. I pulled out my planning tool and together with his regular audiologist we developed the following plan.
A final point I wish to make is that this treatment plan does not need to be executed in one visit. In fact, it would be an overwhelming amount of information to process. However, one can introduce the overall plan initially so the patient can see the journey we are about to embark upon.